Objective: To explore the association of histological subtypes with clinical characteristics and prognosis of patients with sarcoma.
Methods: Data on adult patients with sarcoma was retrieved from the Surveillance, Epidemiology, and End Results (SEER) database (2000-2020). We conducted comparative analyses to describe the differences in clinicopathological features among sarcomas with different histological subtypes, for which propensity score matching (PSM) analyses were utilized to eliminate confounding factors. The COX proportional models were manipulated to identify prognostic variables associated with divergent subtypes of sarcoma.
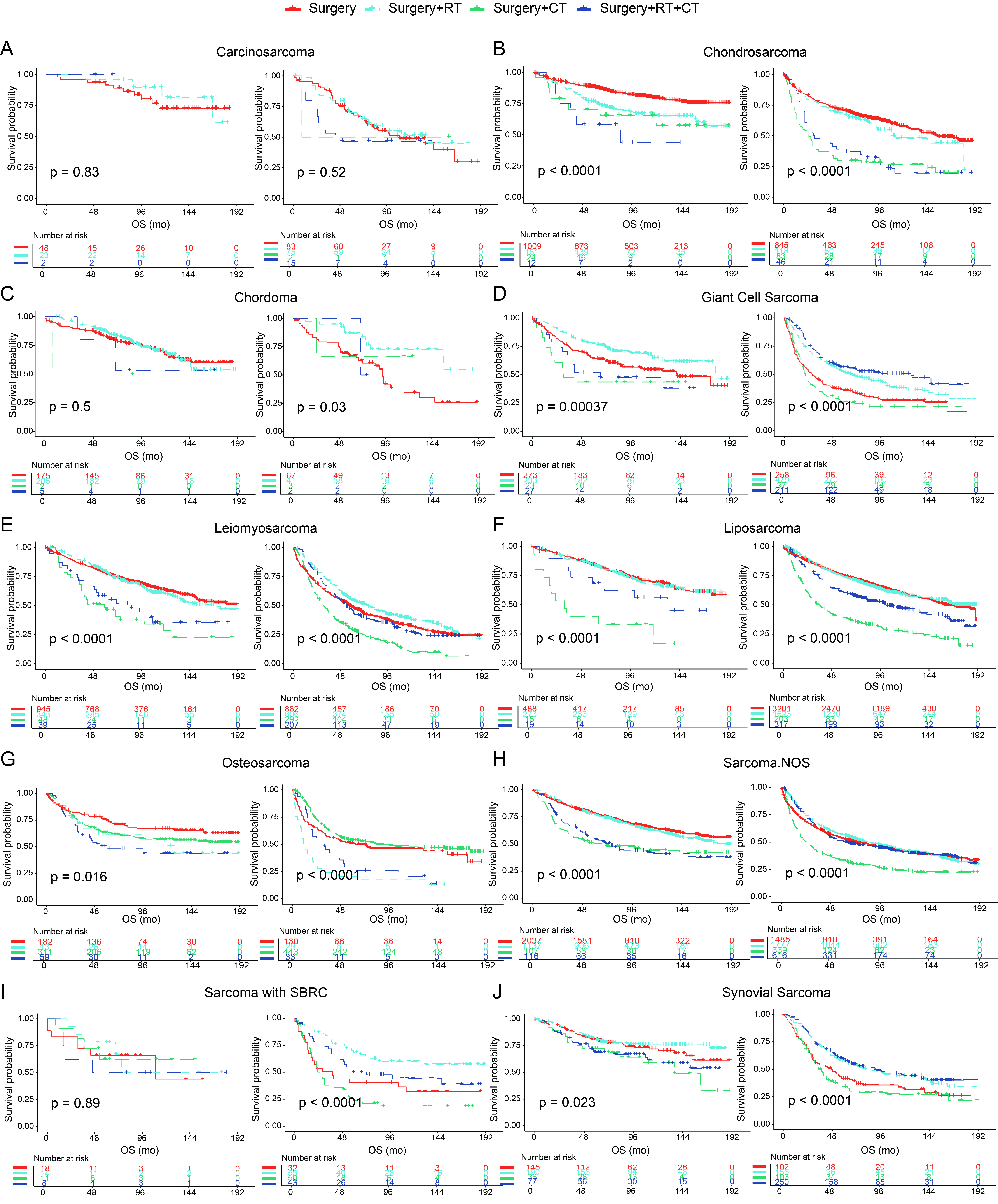
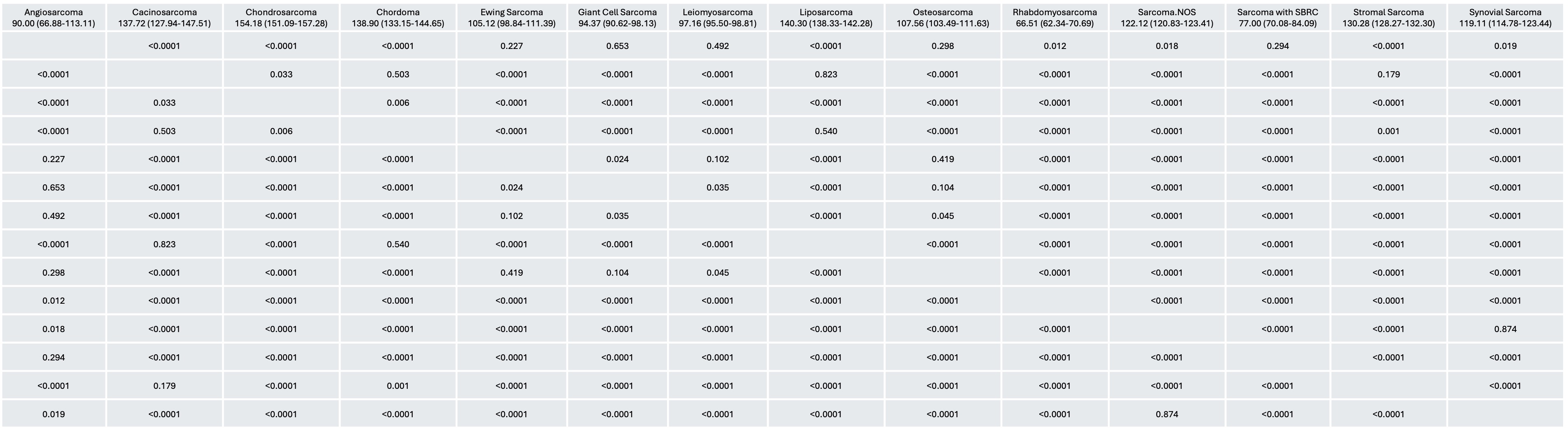
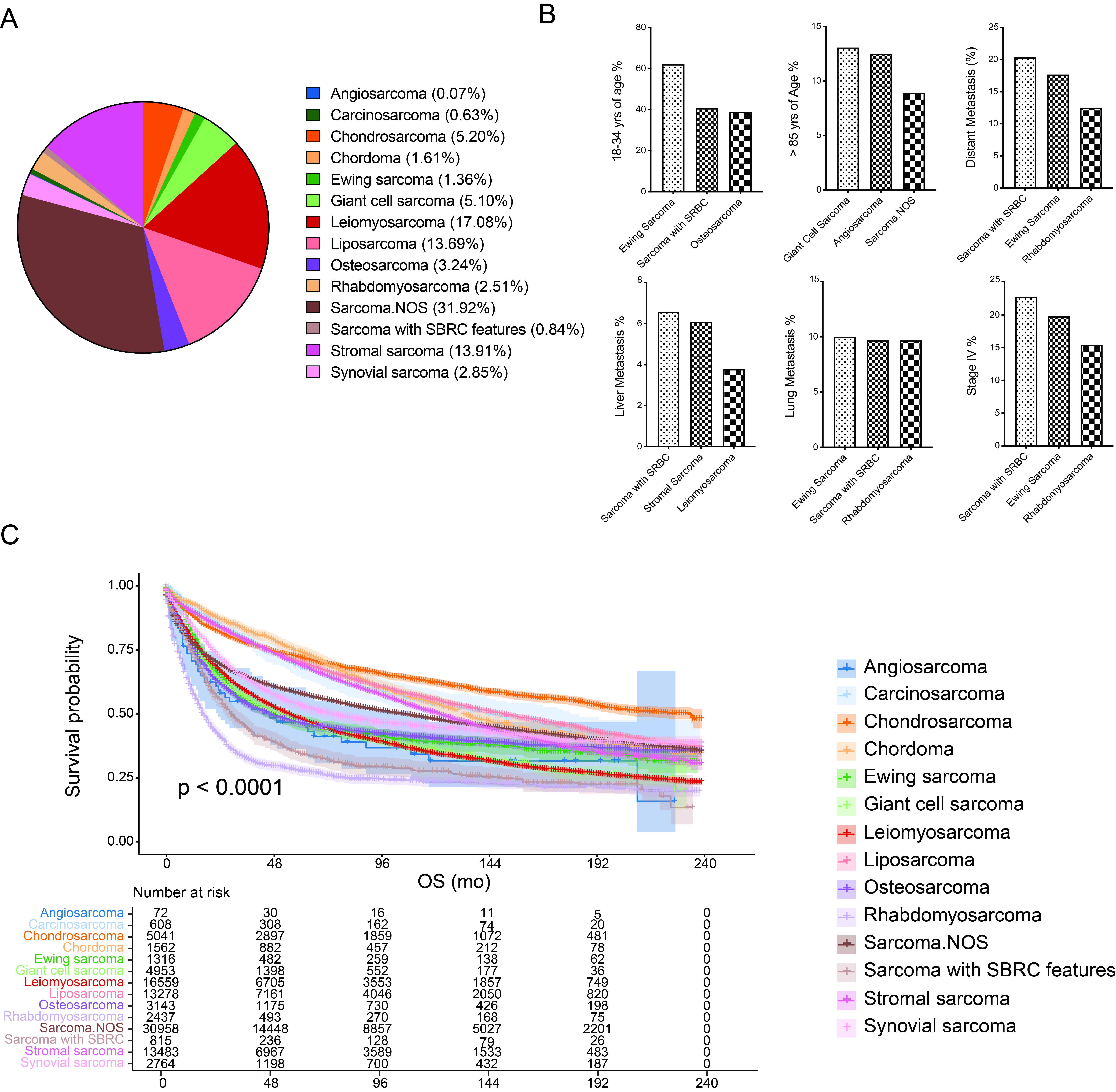
Results: A total of 97062 patients with sarcoma were enrolled, which included 14 histological subtypes comprising angiosarcoma (72, 0.07%), carcinosarcoma (608, 0.63%), chondrosarcoma (5043, 5.20%), chordoma (1562, 1.61%), Ewing sarcoma (1316, 1.36%), giant cell sarcoma (4953, 5.10%), leiomyosarcoma (16574, 17.08%), liposarcoma (13286, 13.69%), osteosarcoma (31.44, 3.24%), rhabdomyosarcoma (2439, 2.51%), sarcoma not otherwise specified (30980, 31.92%), sarcoma with small blue round cell (SBRC) features (815, 0.84%), stromal sarcoma (13505, 13.91%), and synovial sarcoma (2765, 1.85%). De novo liver metastasis mostly occurred in patients with sarcoma with SBRC (6.60%), stromal sarcoma (6.10%), and leiomyosarcoma (3.80%), while lung metastasis at the time of diagnosis tended to occur in Ewing sarcoma (10.00%), sarcoma with SBRC (9.70%), and rhabdomyosarcoma (9.70%). Patients with chondrosarcoma presented the longest median overall survival (mOS) of 158.1 mo (95% CI, 151.1-157.3 mo), followed by liposarcoma (140.4 mo, 95% CI, 138.3-142.3 mo), and chordoma (138.9, 95% CI, 133.2-144.7 mo). By contrast, the shortest mOS was demonstrated in rhabdomyosarcoma (66.5, 95% CI, 62.3-70.7 mo), sarcoma with SBRC (77.0, 95% CI, 70.1-84.1 mo), and angiosarcoma (90.0, 95% CI, 66.9-113.1 mo). Overall, the prognosis of primary sarcoma was significantly better than that of treatment-induced disease (119.0 mo vs. 45.0 mo, P< 0.0001); this tendency remained constant with those comparisons among individual subtypes with the exception of Ewing sarcoma (P=0.11). For patients with giant cell sarcoma, surgical intervention plus radiotherapy provided mOS benefits (P< 0.0001) for all patients; chemotherapy only benefited those with tumor size > 5cm (P< 0.0001). Combination of radiation therapy and surgery versus surgery alone showed comparable mOS for patients with liposarcoma; however, this combination treatment could be the better choice for chordoma (P=0.03), leiomyosarcoma (P< 0.0001), and sarcoma with SBRC (P< 0.0001) with the tumor size > 5cm, in addition to synovial sarcoma with tumor size < 5cm (P=0.023).
Conclusion: Different histological subtype was associated with substantial heterogeneity of clinical features. Individually-tailored treatments should be planned taking into consideration multiple risk factors according to the respective histological subtypes.

 photo")